

Alison wasn’t that worried when her 21-month old daughter Andrea started having a low grade fever of around 38.5°C on January 9 last year. But by the next day, when the fever shot up to 41°C, Alison became alarmed.
“Andrea was cranky all day and refused food and drinks,” recounts the mother. “So I rushed her to the paediatrician near my house who diagnosed the illness as nothing more than a viral fever.”
The doctor did, however, advise Alison to send Andrea for a blood test for Dengue if the fever persisted beyond five days but as Alison recalls, “there was no mention of Kawasaki Disease (KD) and we were not told to look out for its symptoms”.
Alison then brought Andrea home thinking fever medicine would be enough to bring down a viral fever.
By January 11, however, rashes had spread all over Andrea’s body.




“The fever was inconsistent though,” recalls Alison. “It subsided after every dose of medicine so we didn’t think it was anything serious. We thought the rashes would have to run its course before recovery could take place. Besides, Andrea was active and playing around despite being unwell and having no appetite, although there were also many cranky moments in between.”
On January 12, with Andrea still refusing food and drink and showing increasing difficulty at taking her meds, Alison decided to take her daughter to her regular hospital paediatrician.
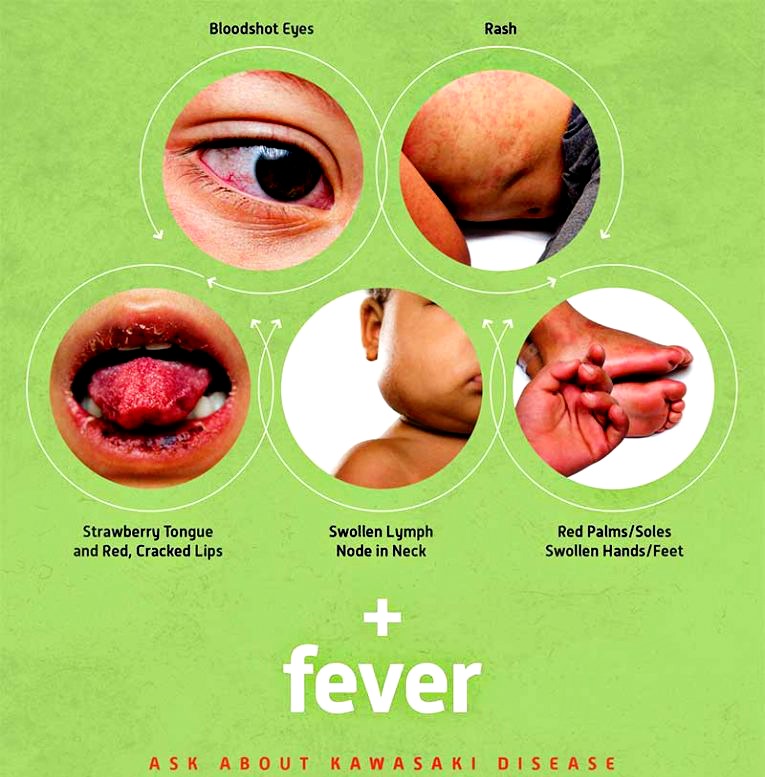
Upon consultation, the doctor said it was likely to be KD as Andrea was showing four of the six symptoms: fever, rashes, a red “strawberry” tongue and bloodshot eyes.
The little girl underwent a blood test and it was confirmed that she had Kawasaki Disease.
“We knew nothing of this disease and were naturally scared when we heard its name. We were told that Andrea would need to go through Intravenous immunoglobulin (IVIG) and would require eight vials to be completed within 24 hours.”


[dropcap letter=”T”]he thing about KD is that no one knows much about it except that it is a serious disease discovered by Japanese paediatrician Tomisaku Kawasaki back in 1967. According to the Kawasaki Disease Foundation which strives to create awareness for this little-known disease through the commemoration of Kawasaki Disease Awareness Day on every January 26, KD primarily affects young children under the age of five, and is more prevalent among children of Asian and Pacific Island descent, although the disease also affects all racial and ethnic groups.
The real danger of KD is that apart from the prolonged fever, redness and swelling, it can also affect the child’s heart if not caught in time.
Motherhood turns to Dr Liew Pei Sze, Consultant Pediatrician from ParkCity Medical Centre to find out more:
- Q1: What is the cause of KD, how prevalent is it in Malaysia and what age children are most susceptible? Is it transmittable to other children?
Dr Liew: The cause of KD is unknown. It is possibly triggered by infection in genetically susceptible children. There is no prevalence data available in Malaysia and it is not a transmittable disease.
- Q2: What are the symptoms? How will parents be able to discern KD from say, a normal fever?
Dr Liew:
1.First phase
High fever lasts more than five days , red eyes without discharge, red and cracked lips, red and strawberry-like tongue, red and swollen hands and feet, body or genital rashes, swollen neck lymph nodes and irritability or poor appetite.
2.Second phase
Skin peeling on hands and feet, diarrhoea, vomiting or abdominal pain.
3.Third phase
All signs and symptoms start to disappear unless complications develop. It may take up to eight weeks for child’s energy level to get back to normal.

- Q3: How dangerous is KD? Is it fatal?
Dr Liew: KD can be fatal in about 1-2% of the affected children even with treatment.
- Q4: Can the disease be cured and what are the long term effects?
Dr Liew: Yes, it can be cured. Treatment started within 10 days from onset of the disease will greatly reduce the chance of long-term heart complications.
KD is the main cause of acquired heart disease in children. It can cause inflammation to vessels (coronary arteries) that supply blood to the heart, which may lead to the formation of aneurysm (vessel with widened and weak wall). The aneurysm can potentially lead to a heart attack or severe internal bleeding.
- Q5: What is the course of treatment? How long would it take? Can it be prevented or inoculated against?
Dr Liew: The main treatment is Immunoglobulin which is administered via a drip through a vein. In addition, oral aspirin is also given to reduce inflammation initially, and later to prevent blood clot formation. At present, there is no way to prevent it.
- Q6: What is your advice to parents?
Dr Liew: Look for a paediatrician in a hospital for further investigation in any children with persistent high fever (T > 38.5° C) for five days or more. Those with any symptoms described in the first phase (under question 2) with high fever more than three days should seek a paediatrician earlier.
