

With World Breastfeeding Week 2019 having been successfully held across 120 countries around the globe from August 1 this year, much has once again been promoted about the benefits of breastfeeding. While a lot of narrative has been added to the latest campaign, some of the old standing problems remain, such as pain during breastfeeding.
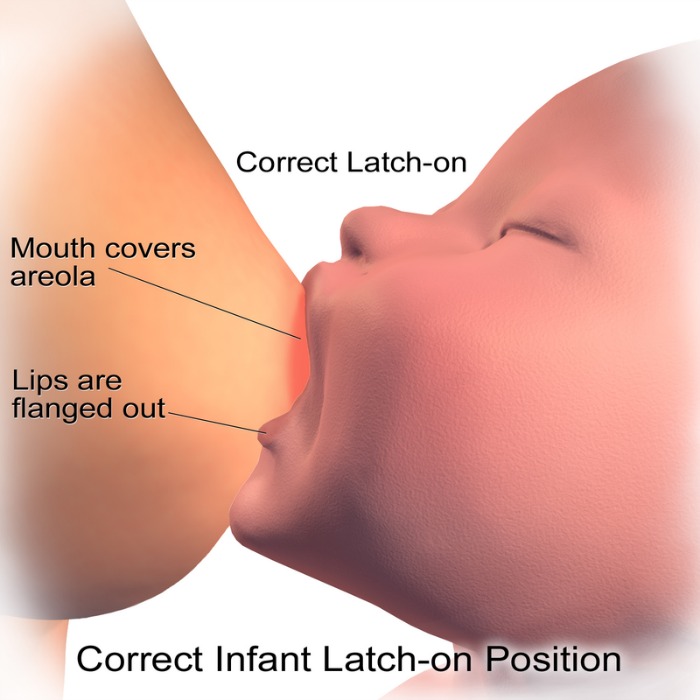
Apparently, this is due to an incorrect latch. If the nipple is not placed deep enough inside baby’s mouth, baby’s gums will only be clamping or “chewing” on the protruding tip of the breast or nipple and cause pain.
Not only that, shallow latching can cause ineffective suckling leaving baby underfed and you with painful sore nipples, clogged milk ducts and even mastitis. This could quickly put paid to the whole breastfeeding endeavour.
Obviously then, the key to successful breastfeeding lies in getting the latch right where enough of your breast tissue must be inside baby’s mouth in order that he gets to compress all the right parts to squeeze out the milk into his throat.

What is a Latch?
To get the latch right, you must first understand what it is.
Latching or a breastfeeding latch refers to how a baby fastens onto the breast when he starts to nurse. A good, deep latch promotes high milk flow and minimises nipple discomfort for the mother, says Wikipedia. A poor latch, on the other hand, results in poor milk transfer to the baby and can quickly lead to sore and cracked nipples.


The Mechanics of Breastfeeding
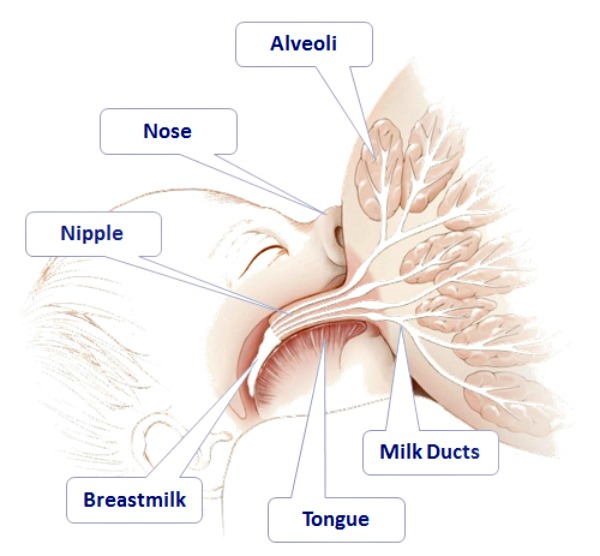
The mechanics of breastfeeding are quite straightforward. Baby will stick out his tongue to feel for the nipple and then use his jaw, tongue, lips and facial muscles to create a vacuum around your breast to breastfeed. He has to take in enough of the areola (the brown ring surrounding the nipple) into his mouth to enable him to work his jaws to compress the breast with her gums. It is the up and down pressure of his jaw and tongue on the areola alongside the vacuum suction in the mouth that squeezes the milk into her throat.
This action of emptying your breast milk signals your body to continue to make more breast milk, which is why breastfeeding has to be done very regularly to establish continued supply.
Here is an excerpt from The Complete Book of Breastfeeding by Sally Wendkos Olds, Laura Marks, MD & Marvin S.Eiger MD that explains how your baby extracts milk from your breast.
![]()

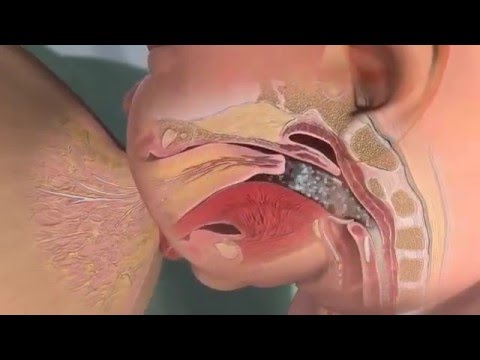
“He starts to suckle by curving up the front of his tongue and then closing his mouth around your breast, raising his lower jaw. He holds the breast between his upper gum and his tongue (which remains over the lower gum throughout the nursing session) and stretches the nipple to at least twice its nesting length. (Fortunately, nipples are elastic). As he moves the back of his tongue downwards, he creates a vacuum inside his mouth. Through the suction created by this negative pressure, he is able to extract milk. This longer nipple extends far into his mouth but moves only a little as he sucks. His tongue still covers his lower gum. The sides of his tongue fold around your nipple, forming a trough; your nipple lies in this trough like a hot dog inside a bun. As the baby sucks on the nipple and much of the areola, the vacuum inside his mouth increases. As the vacuum increases, milk flows from the ducts inside the breast to the nipple, making it available to the baby, who then sucks the milk into his mouth. The milk is carried along inside the baby’s mouth by a rollerlike wave along the top of his tongue which is underneath your elongated nipple. After the milk exists from the milk pores at the tip of your nipple, it goes to the back of your baby’s mouth. For the first five or 10 minutes of nursing, your baby will be suckling forcefully, usually at the rate of one swallow to no more than one or two sucks. After this initial period, the rate may slow down which may signal the need to change him to the second breast.”
![]()
See How Long the Nipple and Areola is pulled into the Back of Baby’s Throat in Order to Breastfeed
How to Latch
- Hold your baby’s whole body close with his nose opposite and level with your nipple. This means his mouth/lips should be slightly below your nipple /areola.
- Remember, a newborns’ head and neck are floppy and need support as you draw him close. Make sure baby’s head and body are in a straight line so that he can swallow easily. Placing a breastfeeding cushion or pillow to support the crook of your arm and baby’s weight in that arm usually helps.
- With your other hand, hold your breast and brush your nipple against his upper lip. This should signal your baby to open his mouth and hang out his tongue in search of food. This is an inborn primeval instinct. The tongue is the “food-seeker” and it should stick out over his bottom gum and lip ready to lap and lick at the food source.
- You baby needs to open his mouth wide as he sticks out his tongue, as wide as he can possibly open it, like a yawn. If he doesn’t open his mouth very, very wide, do not insert your nipple as the latch will be incorrect.
- When his mouth is wide open, quickly stuff as much of your nipple and areola as possible inside his mouth. When he closes his mouth over your breast, his lips should be turned out like a suction cup over the breast. Your baby’s cheeks should look full and rounded as he feeds.

*Note: Baby’s Tongue-Tie
The tongue is a very important feature for successful breastfeeding. Quite a number of babies (as much as 13%) are born with tongue-tie. This is when the frenulum (the thin tissue that connects the bottom of the tongue to the floor of the mouth) stops his ability to move his tongue forward or upward.
Tongue-ties interfere with breastfeeding because baby needs to be able to push his tongue out over his bottom lip, to cup the breast and exert some pressure to extract the milk. When that motion is restricted, the baby’s attempts to get milk often lead to nipple abrasion and damage. It also means baby won’t get enough milk and suffer dehydration and malnutrition.
The problem is easily fixed and is done in the doctor’s clinic/office and not on the operating table. Using no anesthesia or just a topical anaesthetic, the paediatrician cuts the frenulum in a snip or two with sterile scissors and that’s it. The tissue doesn’t have a lot of nerves in it, and won’t bleed much either.
The Two Latch Techniques
Basically, there are two techniques to achieve a proper latch: the Traditional Latch and the Asymmetrical Latch.
1. The Traditional Latch: The traditional latch is as its name suggests. It goes back to the olden days of breastfeeding when baby’s mouth would be centered around the nipple and areola with the nipple pointed straight to the back of baby’s throat. Here, you will see an equal amount of your areola showing all around baby’s mouth.

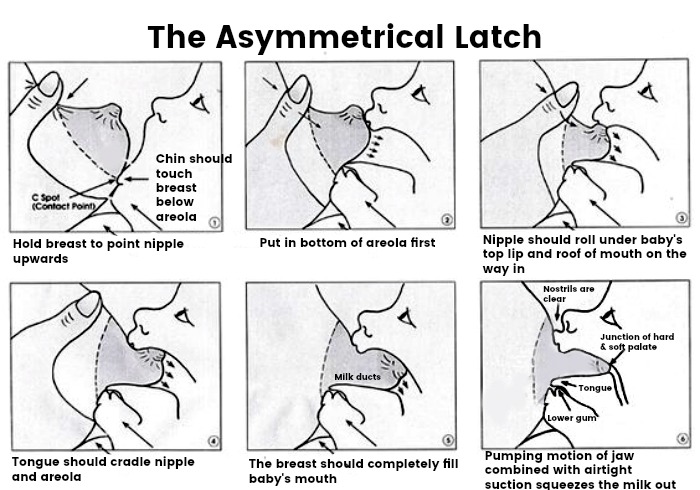
2. The Asymmetrical Latch: The asymmetrical latch is what is promoted nowadays. This technique will aim the nipple upwards to the roof of baby’s mouth (as opposed to the back of his throat in the traditional latch) where the nipple will actually be last to go into baby’s mouth, after you put in the bottom part of the areola. When baby’s mouth is wide open and the tongue is pushed out, bring his chin to touch the breast under the areola and hold your breast in such a way that you point your nipple upwards. Fold in the bottom part of the areola first then release your nipple so that it flips into baby’s mouth brushing under his upper lip and roof of his mouth on the way in. When done correctly, you’ll see more of your areola above baby’s upper lip and less of the areola near the bottom lip and chin when he begins sucking. Baby’s chin will be lightly pressing into your breast and his nose will not be touching your breast at all.
The Asymmetrical Latch is thought to help baby extract milk from the breast more efficiently as the milk ducts are located underneath the areola where the tongue’s action will press out the milk.
Watch How to Achieve the Asymmetrical Latch using the Nipple Flip in this Video

Find the best breast pump for you, only at Motherhood.com.my.